Epidemiology, prevalence, and risk factors
Global trends and prevalence
Narcolepsy is an under-diagnosed sleep disorder that affects 0.03 – 0.16% of the general population in various ethnic groups. It is generally considered as a rare disorder, affecting approximately 1 in 2000 people in the United States. The incidence of narcolepsy can vary by ethnic group. Narcolepsy with cataplexy may be more frequent in Japan: two population-based prevalence studies led to prevalence figures of 0.16% and 0.18% (about 1 in 600 individuals); the lowest rate appears to be in Israel, where it occurs in 1 in 500,000.
The true prevalence of narcolepsy is difficult to determine as some of its clinical, diagnostic, and imaging features overlap with disorders such as depression, epilepsy, psychiatric illness, or other sleep disorders. An accurate diagnosis may often take 10 years after the patient presents with symptoms.
Most cases are sporadic, although genetic predisposition and environmental factors are important for the development of narcolepsy, which is discussed in the next section. In addition, there may be a susceptibility to narcolepsy based on race and ethnicity, as there is a greater incidence of narcolepsy among first-degree relatives. However, it occurs less frequently than would be predicted based on normal patterns of inheritance; in twins, 25 – 31% of monozygotic twins were concordant for narcolepsy with cataplexy, which suggests an interaction of environmental factors and genetic background.
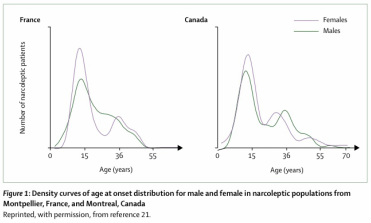
Age of onset: The age of onset of narcolepsy has a bimodal distribution, with peaks that tend to occur around 15 years of age, and then a lesser peak around 36 years. In most cases, narcolepsy presents most commonly before age 25, and usually in the first two decades of life.
Gender: On the whole, men and women seem to be equally affected, although there are conflicting studies as to which gender is more affected by narcolepsy.
Risk factors: Risk factors of developing narcolepsy have yet to be identified, as research into established risk factors is lacking. A case-control study examined possible environmental risk factors, and identified the following as possible risk factors:
- Flu infections and unexplained fevers
- Life stressors and major changes in sleeping habits
- Exposure to puberty
Factors that have been most studied include body mass index, immune responses and stressful life events. However, these factors may reflect a consequence rather than a cause of disease. Other postulations include head trauma or injury, month of birth and having suffered meningitis or encephalitis in the past.
References
1. Ahmed I, Thorpy M. Clinical features, diagnosis and treatment of narcolepsy. Clin Chest Med 2010; 31: 371 – 381
2. Dauvilliers Y., Arnulf I, Mignot E. Narcolepsy with Cataplexy. Lancet (Seminar) 2007; 369: 499 – 511
3. Nishino S. Clinical and neurobiological aspects of narcolepsy. Sleep Medicine 2007; 2: 373 – 399
4. Robinson, Keating. Sodium oxybate in the management of narcolepsy. CNS Drugs 2007.
Images:
Dauvilliers Y., Arnulf I, Mignot E. Narcolepsy with Cataplexy. Lancet (Seminar) 2007; 369: 499 – 511 http://bouldersleeptherapy.com/disorders/narcolepsy.php/
autoimmunediseasesa2z.com
www3.unil.ch
